Diabetes affects approximately 3-4% of the British population but is thought to be significantly under-diagnosed. How can we improve the number of patients who are diagnosed early and so improve their risk of long-term complications?

Making Best Practice, Every Day Practice

This resource is fully searchable using the search box at the top of the page, or to narrow down your selection using filters click on 'Knowledge hub' in the main navigation.



More than 4.9 million people in the UK have diagnosed diabetes and by 2030 Diabetes UK estimate there will be 5.5 million people with diabetes.
The care of patients with diabetes – particularly type 2 diabetes which counts for about 90% of patients seen in primary care – is a significant challenge.
Our resources focus on:
![]() Detection of pre-diabetes conditions frequently associated with obesity and metabolic disorders
Detection of pre-diabetes conditions frequently associated with obesity and metabolic disorders
![]() Early diagnosis of type 2 diabetes
Early diagnosis of type 2 diabetes
![]() Interventions to reduce the risks of cardiovascular and renal disease (the cardio-renal syndrome)
Interventions to reduce the risks of cardiovascular and renal disease (the cardio-renal syndrome)
![]() Glycaemic control with established therapies including metformin
Glycaemic control with established therapies including metformin
![]() The roles for newer agents including SGLT2 inhibitors and DDP-4 inhibitors
The roles for newer agents including SGLT2 inhibitors and DDP-4 inhibitors
![]() Importance of lipid (cholesterol) management and antihypertensive therapy
Importance of lipid (cholesterol) management and antihypertensive therapy
Additional contributions discuss:

![]() The initiation and intensification of insulin in people with type 2 diabetes
The initiation and intensification of insulin in people with type 2 diabetes
![]() Diagnosis and management of people with type 1 diabetes
Diagnosis and management of people with type 1 diabetes
![]() Prevention of hypoglycaemia
Prevention of hypoglycaemia
Diabetes affects approximately 3-4% of the British population but is thought to be significantly under-diagnosed. How can we improve the number of patients who are diagnosed early and so improve their risk of long-term complications?
Glycated haemoglobin – HbA1C, or A1C as it is now being called – should be used to diagnose diabetes, according to a recent recommendation from an international expert committee appointed by the American Diabetes Association, the International Diabetes Federation and the European Association for the Study of Diabetes. We explore the basis for this recommendation, and look at why HbA1C would provide a more accurate measure for diagnosing diabetes than glucose tests and what the change would mean in clinical practice.
Glycated haemoglobin – HbA1C, or A1C as it is now being called – should be used to diagnose diabetes, according to a recent recommendation from an international expert committee appointed by the American Diabetes Association, the International Diabetes Federation and the European Association for the Study of Diabetes. We explore the basis for this recommendation, and look at why HbA1C would provide a more accurate measure for diagnosing diabetes than glucose tests and what the change would mean in clinical practice.
Diabetes affects approximately 3-4% of the British population but is thought to be significantly under-diagnosed. How can we improve the number of patients who are diagnosed early and so improve their risk of long-term complications?
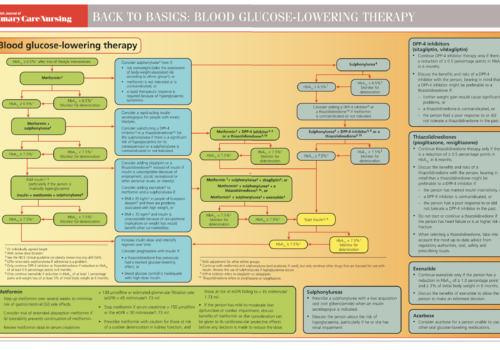
In May 2009, NICE published recommendations on the use of newer agents for the control of blood glucose in type 2 diabetes. This guideline provides a partial update for NICE Clinical Guideline 66 on the management of type 2 diabetes that was published last year. These newer agents include the dipeptidyl peptidase-4 (DPP-4) inhibitors, thiazolidinediones (TZDs), the glucagon-like peptide-1 (GLP-1) mimetic exenatide and the long-acting insulin analogues (insulin detemir and insulin glargine).
The new NICE guideline enables us to individualise care bearing in mind the needs of the person in front of us. It is concerned with clinical efficacy, and – for once – the cost of care has not noticeably influenced its recommendations. In contrast, QOF does the exact opposite, demanding that we drive our patients’ HbA1c down to low […]
Many people with type 2 diabetes are overweight or obese at diagnosis and continue to struggle to control their weight. This article looks at why people with diabetes find weight control more of a challenge than the rest of us and how practice nurses can help patients to remain positive, particularly when starting insulin to optimise blood glucose control.
The new national strategy for vascular risk assessment, now being referred to as NHS Health Check, will include testing for diabetes and impaired glucose tolerance (IGT). This follows a major evaluation of the evidence showing that it is more cost-effective to screen individuals for IGT than screening for diabetes alone, but only as part of the broader vascular risk assessment. This article examines the concepts of IGT and impaired fasting glucose (IFG) and offers practical advice as to how these conditions can be managed in primary care.














A unique new e-platform for primary care

By continuing to this site you are confirming that you are a healthcare professional and are opting into the use of cookies.