There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
Making Best Practice, Every Day Practice


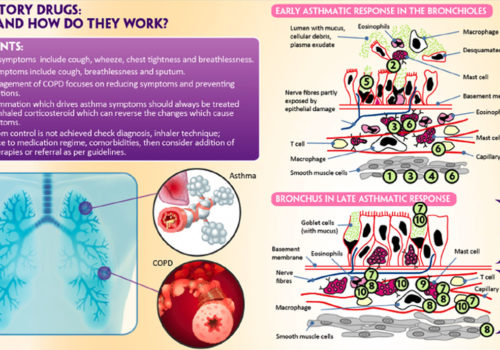
About asthma and allergies
Asthma and allergies result in multiple long term consultations with an estimated 1 in 12 adults and 1 in 11 children in the UK. Sadly death rates remain stubbornly high will an average of three deaths a day.
Currently asthma costs the NHS about £1 billion p.a. and results in about 80,000 hospital admissions.
Allergy is affecting an increasing number of British adults and today they affect up to 44% of the population. Most allergies are not life threatening but in severe cases they cause anaphylaxis which may be fatal.
These resources include:
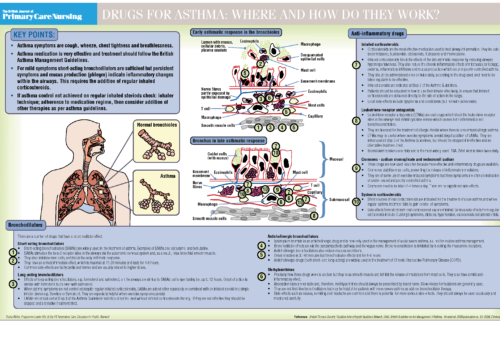
![]() Explanations of the etiology of asthma and triggers of acute asthma attacks
Explanations of the etiology of asthma and triggers of acute asthma attacks
![]() The spectrum of asthma medications including inhaled corticosteroids, long-acting beta agonists (LABAs), leukotriene modifiers and inhalers combining a corticosteroid and a LABA
The spectrum of asthma medications including inhaled corticosteroids, long-acting beta agonists (LABAs), leukotriene modifiers and inhalers combining a corticosteroid and a LABA
![]() Reviews of recent asthma management guidelines and their application in primary care
Reviews of recent asthma management guidelines and their application in primary care

![]() Techniques and guidance to improve inhaler technique in children and adults
Techniques and guidance to improve inhaler technique in children and adults
![]() Articles also discuss common allergies such as allergic rhinitis and urticaria and the safe use of antihistamines
Articles also discuss common allergies such as allergic rhinitis and urticaria and the safe use of antihistamines
There are several different drug types used in the management of hypertension. This back to basics provides a useful summary of the different antihypertensive drug classes and how they act to regulate blood pressure.
Asthma affects more than 5 million
people of all ages in the UK today.
The vast majority of asthma is
diagnosed and managed in primary
care and most people with asthma rarely need
to see a hospital specialist. Until recently it
has been difficult to measure the level of
inflammation seen in asthma accurately in
general practice. However, new techniques
such as exhaled nitric oxide measurement are
now available for use and this article provides
GP and nurse perspectives on the potential of
such techniques in primary care.
Asthma medications should routinely be delivered by a pressurised metered dose inhaler
(pMDI) and spacer system, with a facemask where necessary, in children under five,
according to the National Institute for Health and Clinical Excellence (NICE).1
For older children, aged 5-15 years, NICE has advised that a child’s therapeutic needs,
the ability to develop and maintain an effective technique, the suitability of a device for the
child’s and carer’s lifestyles (ie portability and convenience) and the likelihood of good
compliance are the factors that should govern the choice of device.2 Only once these factors
have been taken into account, should choice be made on the basis of cost minimisation.
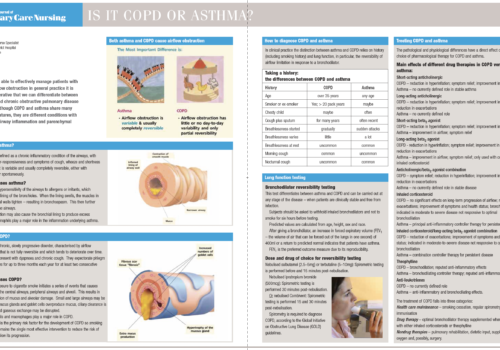
To be able to effectively manage patients with
airflow obstruction in general practice it is
imperative that we can differentiate between
asthma and chronic obstructive pulmonary disease
(COPD). Although COPD and asthma share many
clinical features, they are different conditions with
different airway inflammation and parenchymal
patterns.
Patients with allergic asthma, intermittent (seasonal) or persistent (perennial) allergic
rhinitis, represent a significant proportion of primary care consultations. There is
growing awareness of allergy and the possibility of an allergic component as the cause
of a wide variety of symptoms. It is important to understand how to diagnose atopy to
ensure appropriate management and care of our patients. Diagnosing allergy is initially about
asking the right questions, followed by confirming or refuting the diagnosis by objective testing.
In this article, we explore history taking and objective testing that will help us to manage and
advise patients appropriately.
Asthma is a common condition in children, with approximately one in eight youngsters in
the UK receiving treatment for asthma at any given time. The British guidelines on the
management of asthma have separate pathways for children of different ages, for those
under 5 and for children aged 5-12 years. In this article, we review some of the
challenges of treating children with asthma, in particular, the best use of bronchodilators.
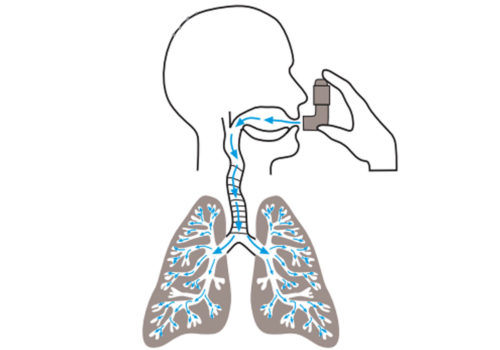
Asthma UK estimates that 2.1 million patients in the UK are suffering unnecessarily because
they do not use their asthma treatment effectively. This article looks at how inhaled
therapies are deposited in the lungs, and at the basic differences between inhalers – with
a focus on optimising inhaler technique.
The current treatment of asthma in the UK is rightfully seen as a triumph of chronic disease management within a primary care setting. Almost all routine asthma care and, increasingly, elements of acute asthma care, are now provided in general practice. Over the past twenty years, significant effort and investment have gone into the production […]
One person in every five households in the UK is receiving treatment for asthma,
according to latest figures. As well as treatment for asthma, many of these individuals
also self-medicate for minor illnesses or require prescribed medication for other
conditions. It is important that the drugs they take do not adversely affect their asthma
control. In this article we review which drugs might cause problems in patients also taking
treatment for asthma.
Asthma is a chronic disease that has, for a long time, been the domain of primary care nurses, and many have qualifications enabling them to run nurse-led asthma clinics. It is, therefore, essential to fully understand the Quality and Outcomes Framework (QOF) and to be able to maximise the points available to the practice, at the same time as providing a comprehensive service to patients. In this article, we review the QOF indicators for asthma, strategies for optimising record keeping and performing asthma reviews.
More than half of people with asthma in the UK have inadequate symptom control,
despite the range of effective therapies now available. Rather than blaming
patients when they fail to take their medications as prescribed, we need to
examine the way we conduct asthma consultations and ask whether we are failing
to meet the needs of individual patients. How can we gain greater understanding about what
people with asthma want from healthcare professionals and treatments, so we can achieve a
more patient-centred approach to care?














A unique new e-platform for primary care

By continuing to this site you are confirming that you are a healthcare professional and are opting into the use of cookies.