Healthcare professionals spend a great deal of their time screening for, and treating, silent killer diseases such as diabetes, hypertension and hyperlipidaemia but often ignore the primary cause of these conditions, which is often – quite literally – staring them in the face. Obesity can be seen without the need to use any fancy gadgets – we simply need to use our eyes each time we see a patient. There are essentially two main body shapes – apples and pears – each associated with different distributions of body fat. Pearshaped people carry most of their excess fat around the hips, buttocks and thighs. Apples carry most of their excess body fat around the middle; this is known as central obesity and is much riskier for diabetes and cardiovascular disease. In this article we review why central obesity matters, how to measure it and management strategies.
Acute coronary syndromes
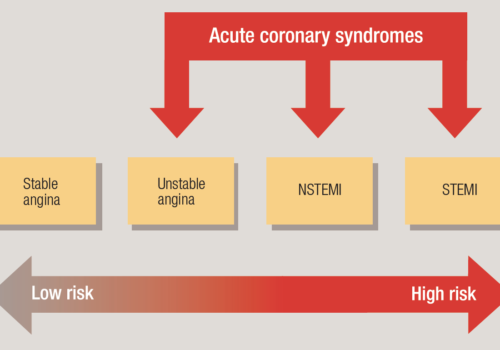
Acute coronary syndromes (ACS) include common and high-risk conditions such as unstable angina, which can be difficult to diagnose, particularly in women, the elderly and diabetics. Early identification and appropriate management can significantly reduce the risk of death, morbidity and subsequent hospital admissions. This article aims to clarify what happens in ACS, how they present and how they should be managed.
Editorial
Welcome to the latest issue of the British Journal of Primary Care Nursing (BJPCN). The NHS is currently in meltdown around the ears of primary care teams, with new mergers and reshuffles. There is great uncertainty about who will lead the new PCTs and the structures that will support the delivery of CHD and diabetes care. But, like many of you, I have been around long enough to know that things ‘go in circles’.
Validating and maintaining your CHD register
Disease registers are essential for practices to optimise the diagnosis, management and follow-up of patients with a particular condition, in addition to being an important feature of the Quality and Outcomes Framework. Practices are responsible for demonstrating that they have systems in place to maintain a high-quality register. In this article, we look at a ‘recipe’ for validating a coronary heart disease (CHD) register – but the same method used for validating and maintaining the register can apply to any disease, using appropriate diagnostic and treatment information.
Type 2 diabetes in south Asian communities in the UK
People from ethnic minorities may not get the diabetes care they need because of issues associated with language, literacy and culture, warned a recent Audit Commission report on diabetes – Testing Times. This article explores these issues and gives some insight into the challenges of looking after South Asians – Bangladeshis, Pakistanis, Indians and Sri Lankans – with diabetes, as well as offering some pointers to improve their care and treatment.
Keep taking the tablets: achieving adherence in type 2 diabetes
Most patients with type 2 diabetes require many tablets to control their diabetes and prevent cardiovascular complications. Patients are often prescribed two or three antidiabetic agents, two or three antihypertensives, one or more lipid-lowering tablets and low-dose aspirin. Research has warned that fewer than 50% of patients take their prescribed diabetes medication adequately. The consequence of this poor adherence is increased risk of cardiovascular complications. How do we help patients to take their tablets and so improve their health and long-term outcomes?
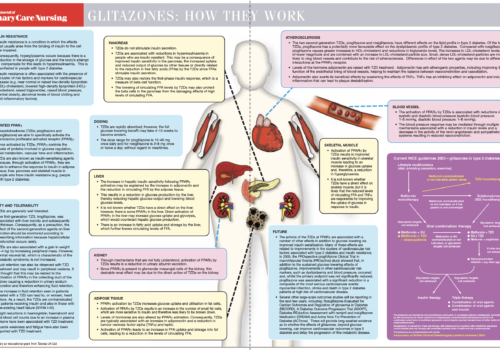
Back to Basics: Glitazones: how they work
Monitoring kidney function in the surgery
The most common cause of chronic kidney failure is diabetes, which accounts for between 30 and 40% of all cases. Chronic kidney disease is a long-term condition usually taking between fifteen and twenty years to reach the final stages. Although 30% of all people with type 2 diabetes will develop some degree of kidney disease, only a minority go on to develop end-stage renal failure. In this article, we look at the benefits of early detection and treatment in slowing the progression of renal impairment.
The role of dietary fibre in optimising health
The gastrointestinal tract plays a vital – and sometimes overlooked – role in maintaining overall health. Dietary fibre, eaten as part of a balanced diet, helps to ensure effective functioning of the intestines and can offer benefit in terms of the prevention and treatment of a number of health problems. As levels of obesity in the population continue to escalate, research has shown that dietary fibre has an important role in satisfying appetite and in weight management, in addition to playing a potential role in controlling insulin levels.
Metabolic Syndrome: a Cluster of Risk Factors

The metabolic syndrome is characterised by a cluster of metabolic risk factors which may include abdominal obesity, dyslipidaemia, high blood pressure and insulin resistance or glucose intolerance. Patients with this cluster are at increased risk of coronary heart disease, stroke, peripheral vascular disease and type 2 diabetes. The dominant underlying risk factors for the syndrome are abdominal obesity and insulin resistance – so the epidemic of obesity means that we will be seeing a major increase in cases of metabolic syndrome over the next few years. Management requires tight control of all risk factors, with weight loss and prevention of weight gain being important preventive measures.
Back to Basics: Calculating cardiovascular risk: ‘How To’ guide for the new British Guidelines

Calculating cardiovascular risk is at the heart of primary prevention – it gives us a practical way of assessing who we should be targeting with lifestyle changes and drug treatment to reduce the chance of them suffering a heart attack or stroke in the future. The new Joint British Guidelines make it very clear who we should be screening for CVD and how to calculate their risk.
New Joint British Guidelines on CVD Prevention
Nearly 250,000 people die each year in the UK from cardiovascular disease (CVD), despite all the hard work of healthcare professionals. The new Joint British Societies’ Guidelines on Prevention of Cardiovascular Disease in Clinical Practice (JBS2), published recently by all of the leading societies working to reduce CVD in this country, take a ‘get tougher’ approach to further reduce CVD deaths. They widen the range of patients who should be included in primary prevention, in addition to setting lower targets for total cholesterol (4.0 mmol/L), low-density lipoprotein (LDL) cholesterol (2.0 mmol/L) and blood pressure (140/85 mmHg).














